Epilepsy Program in Mozambique
Epilepsy Mission Novembre 8 – 18 2023
Contents
- Epilepsy in Mozambique
- The first video-electroencephalograph installed in Mozambique
- The DREAM epilepsy program in three sub-Saharan countries. A collaboration between DREAM, the Besta Neurological Institute, the Italian Society of Neurology and the Mariani Foundation
- Education and training of clinicians and the WHO-Intersectoral Global Action Plan 2022-2031
- Education and training of community health workers
Epilepsy in Mozambique
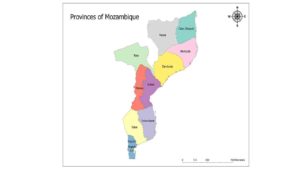
Epilepsy is widespread in Mozambique, affecting 2 percent of the population, ie about a million sufferers (photo 1). Over 80% have no/very poor access to proper diagnosis and treatment. Three millions people live in the province of Sofala, which has Beira as its main city, the second largest in the country; according to previous studies over 90% of people with epilepsy (PWE) in the area do not have access to treatment. Foto 1. Epilepsy in Mozambique.
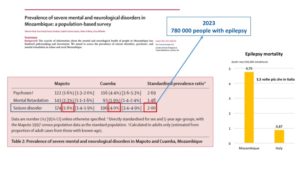
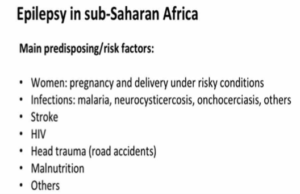
Epilepsy is more prevalent in sub-Saharan African countries as Mozambique compared to Western countries. This is due to specific factors such as small and large traumas that children suffer during childbirth and pregnancy due to the uncomfortable living conditions of many African women, infections as malaria and HIV often invovling the brain, the uncontrolled increase in stroke nowdays among the most lethal and frequent diseases in Africa, the growing number of serious road accidents, malnutrition.
The first video-electroencephalograph installed in Mozambique
The Italian Society of Neurology (SIN) donated a video-electroencephalograph, the first in Mozambique, installed in November 2023 at the DREAM center in Beira.

The DREAM epilepsy program implements the indications of the World Health Organization (WHO) Intersectoral Global Action Plan (IGAP) 2022-2031 which aims to create access to treatment for epilepsy also in accordance with the Sustainable Development Goals.


The DREAM epilepsy program in three sub-Saharan countries. A collaboration between DREAM, the Besta Neurological Institute, the Italian Society of Neurology and the Mariani Foundation
In over 20 years of activity in Mozambique DREAM has built a realiable network to manage chronic diseases such as HIV, hypertension, diabetes and other diseases. The agreements with the Besta Neurological Institute, the Italian Society of Neurology and the Mariani Foundation allow neurologists to use the DREAM network for the management of chronic neurologic disorders as epilepsy. The DREAM-epilepsy program was started in Malawi and Central African Republic, and now also in Mozambique. In the three countries people with epilepsy receive excellence care in 12 DREAM centers; and three of these centers are equipped with videoEEG. This is a sustainable intervention model implementing epilepsy care at primary care level in accordance with national governments.

In Malawi and Central African Republic, DREAM is treating 2000 patients who now live free from the burden of the disease, still seen as a supernatural and contagious phenomenon. The stigma is strong.
The Provincial Director of Sofala, Neusa Rosalina Casimiro Joe, the District Director of Beira, Sonia Ana Mudengue, the Clinical Director of Hospital Central of Beira Ana Nicolau Tambu took part in the inauguration of the videoEEG and the training course. They all had words of appreciation for the initiative. A stable network for staff training and patient management throughout the vast Sofala region and beyond is now active.

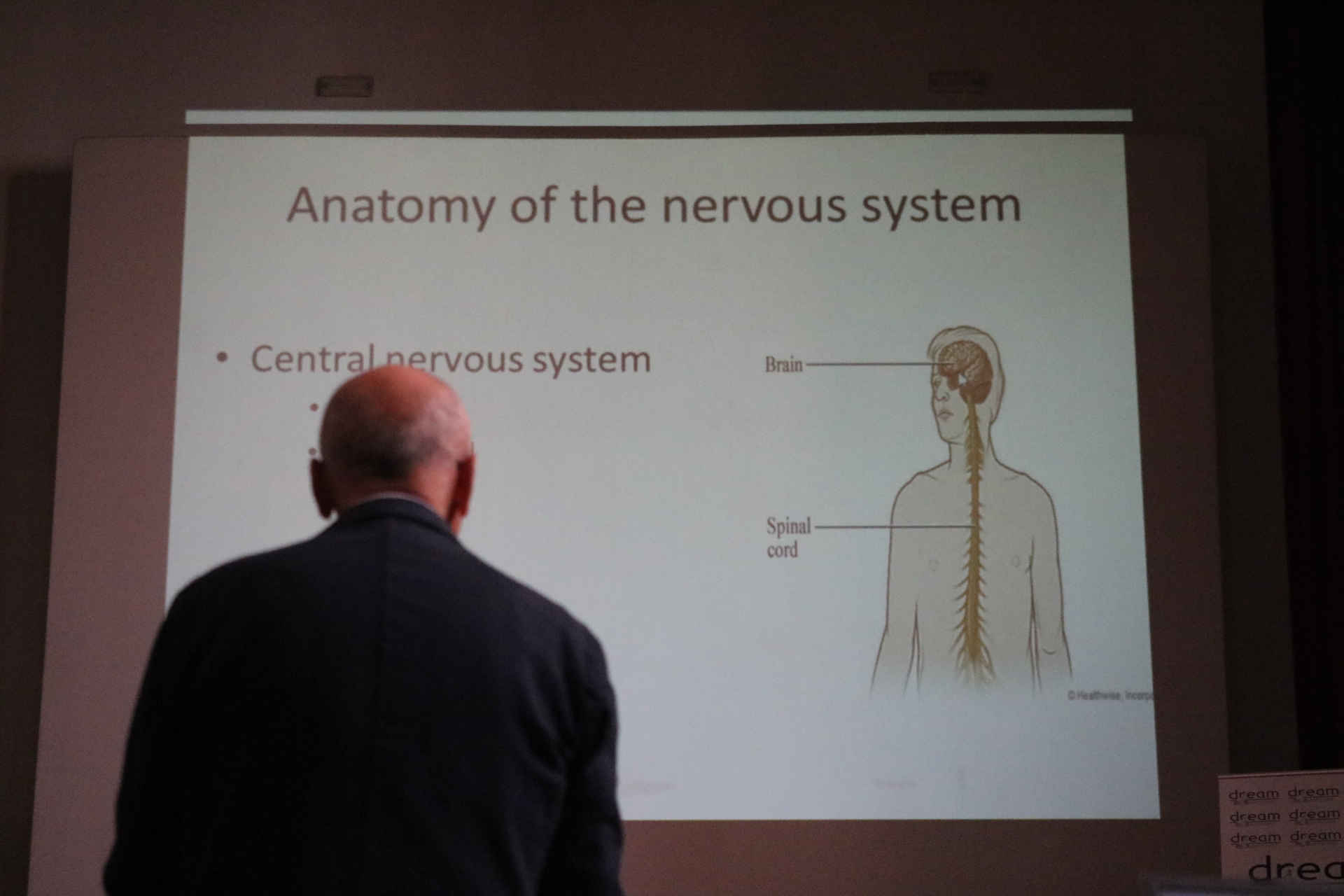
Education and training of clinicians and the WHO-Intersectoral Global Action Plan 2022-2031
Unfortunately, neurologists (specialists for treating epilepsy) in sub-Saharan Africa are very rare, one for every 2.7 million inhabitants, in Mozambique around 12 for 33 million inhabitants. Lack of neurologists will last for the next decades. The Western model of epilepsy care managed by neurologist is not sustainable for sub-Saharan Africa either in the short or medium-long term as the continent does not have the almost 300 thousand euros necessary to train a specialist (this is how much Western countries spend to bring a young person to graduate and then to become neurologist). In addition, the few neurologists in sub-Saharan Africa have a huge hospital workload to not allow them to take care and to follow activities and patients at primary care centres – the so-called mental health centers, government centers where people with epilepsy are sent.
The management of the majority of patients with epilepsy in Africa is performed by non-graduate healthcare personnel (non physician clinicians) whose training in neurology and epilepsy is insufficient.
DREAM offers to NPC and health personnel continuous education according to the WHO task-shifting and task-sharing education and training model while Western academic institutions traditionally offer training to medical specialists working in university-hospital settings.
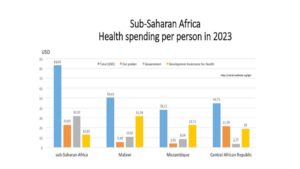
The discrepancy between the resources of sub-Saharan governments for citizen health and the costs of antiepileptic drugs highlights some of the problems also suggesting steps forward.
Sub-Saharan Africa health spending per capita is about 80 dollars in one year to include foreign aid (Development Assistance for Health – DAH). This is not sufficient to cover the costs of a year of treatment with most first-line antiepileptics (in Italy the annual per capita expenditure on health is around 3 thousand euros, ed.). To implement the universal access to care, the WHO-IGAP and SDG, DREAM offers both antiepileptic drugs and healthcare services free of charge – the same DREAM does for HIV and other diseases. Offering free services to people with epilepsy in sub-Saharan Africa is a matter of human rights since over 60% of the population lives below the absolute poverty line, is 1.9 USD per day.
The same principle of social equity is applied in Europe; in Italy the principle is applied as exemption from the ticket for the protection of the less well-off.
Poor training and lack of antiepileptic drugs discourage people with epilepsy from returning to health centers and those who cannot afford to buy medicines at their own expense stop treating the disease. The high costs of transport further discourage sick people from going to the centres, petrol costs almost the same as in Europe compared to meager salaries which are not always guaranteed by a largely informal economy. Many sick people continue to turn to curandeiro or false prophets who promise healing as long as they join sects that sell health and success also using religions as viaticum.
Italian neurologists are involved in education and training courses to local health personnel. Lessons include principles of anatomy and physiology of the nervous system, epidemiology of epilepsy, principles of pathophysiology (photos 10, 11), clinic and treatment, coexistence with other widespread diseases such as HIV, tuberculosis, malaria, discussion of clinical cases (photos 12-14), genesis of brain electrical activity, main EEG waves and pathological pictures, montages and execution of the ‘EEG etc.
Training on the EEG machine (photos 15 and 16) is also important to make the “South-North-South” communication between local operators and remote specialists optimal and efficient.




Education and training of community health workers
Community health workers, activists and nurses paly an important role since they meet patients both before and after medical visits: they listen to what patients sometimes do not report to clinicians and which can be important to fully understand the patient and her/his problems that could barrier returning to the center for checks and resupplying medicines, etc. Community health workers can go for home care, in the villages, bridging health centres and patients’ real life. For this ample space is also dedicated to their training.

During the sessions it always emerges that all the operators have dealt with epilepsy patients despite never having taken part in treatment programs: it happens among relatives, friends, in public places, on the street, at school. From their stories it emerges how widespread and how hidden the disease is.
Among the community health workers there were also those who have been working in the DREAM program for more than 20 years to fight HIV. There are many similarities that have emerged between HIV and epilepsy.
During the meetings, experiences and testimonies emerge that help us to better understand the condition of people with epilepsy; here are reported some of their words (the names are fictitious).
Fear
Antonio: “at the beginning there was a great fear of HIV infection, even on the part of healthcare workers, we were afraid of being with the sick, touching them, as happens today with epilepsy” which is believed to be contagious for the most population.
Building trust in institutions
Talking about of fear about HIV treatment, Elena added: “there was fear that the white man’s treatments could kill us Africans due to a premeditated plan“. The belief has not yet completely passed and Antonio says “Two weeks ago in Nampula (city in the north of the country) for to combat the beginning of a cholera epidemic, an information campaign was held on the streets. A policeman who accompanied the medical team was killed by people who accused the team of distributing drugs that would then kill them.” a deep mistrust in institutions. In a similar way this sometimes also happens with epilepsy. Elena tells of an orphan child with epilepsy, whose grandmother did not want him to take medicine to treat epilepsy.
Lack of medicines lead people to loose trust and to not return to the center also because transport is expensive: “it is difficult that patients and their families listen and follow you when words are not followed by actions, when there is lack of medicines“. The belief that epilepsy is not treatable is perpetuated since there are few sufferers who, being able to benefit from uninterrupted treatments, can then testify the validity of the drugs which in turn generates trust and hope, favoring a change in the culture of the disease. And if treatments are lacking, people turn elsewhere, often to the thriving market of easy cures at the expense of money.
Children
There are many stories of children and young people who are denied access to school because they suffer from epilepsy for fear of contagion. Alberto says “Children with epilepsy are often kept locked up at home. In recent days, national TV has talked about a child suffering from epilepsy who has been segregated at home for some time in Maputo, the capital. Patients’ condition is even worse in rural centers...” “When I was a teenager I had two friends with epileptic seizures, both of whom were banned from attending school. One went to work as a laborer, he was 13 years old, he had turned to traditional medicine without benefits, his face was full of scars from falls caused by seizures“.
Mothers
Anna says “I knew a young pregnant woman with epilepsy; when crises happened to her on the street, for fear of people’s judgement, of the stigma and isolation that would result, she tried to minimize it by saying “it’s nothing”. I was thinking: what if she has a seizure and falls while she is holding and breastfeeding the baby?…” . “A friend of mine fell into boiling oil in the kitchen during a seizure. At the moment she didn’t feel anything but then when she regained her senses… “.
Knowledge and responsibility.
Antonio, DREAM activist, had participated in our training course eight months ago; he remembered the description of epilepsy very well even though he had never studied it before: “a sudden and short-lived electrical discharge in the brain” he promptly said.
Memory and words open up a new culture, and the parallel with HIV is quite impressive: “20 years ago” he says “the word viral load and its meaning were obscure to people; then these terms gradually entered the lives of patients because they accompanied a change; a change that was previously thought impossible but which, thanks to the accessible treatment, always available, had become possible, visible, we could touch it with our hands, on our skin“.
Viral load and electrical discharge in the brain are technical words but little by little, thanks to loyal and continuous accessible those estranger words have now a meaning for the patients: the fear is gone, the trust is borne.
Patients are now aware of the disease and even more responsible for their own health; and that of others.
It was like this for HIV: we dream it also for epilepsy.

